

When a family walks into your clinic, what do you assess first? It’s a deceptively simple question and it was the one Renee Collins, BCBA, CBA, and Developmental Educator at Super Kids Behavioural Consulting, put to her audience at the Connected Care Conference 2026 in Sydney.
Her answer challenged practitioners to think beyond behaviour plans and skill acquisition programs, and to look first at the health behaviours that are often the silent drivers of everything else: sleep, feeding, toileting, exercise, and leisure. This is a summary of the key insights from her presentation.

Renee opened with a grounding reminder: the challenges she was about to discuss including behavioural sleep disorders, food selectivity, toileting difficulties, are not edge cases. They are the lived reality of the families sitting in front of us every day. Her audience included BCBAs, behaviour support practitioners, and developmental educators working primarily with autistic individuals, people with intellectual disabilities, and toddlers with developmental disabilities. For these populations, health behaviour challenges are pervasive, underaddressed, and deeply consequential.
The Framework: Health Behaviours Come First
Central to Renee’s presentation was a powerful reframing of clinical priority. Using a pyramid visual, the base being health and daily living skills (sleep, eating, toileting, leisure, communication, exercise), and the apex labelled “everything else” — she made the case that practitioners consistently get the order backwards. We spend our time on the top of the pyramid while the foundations remain unstable.
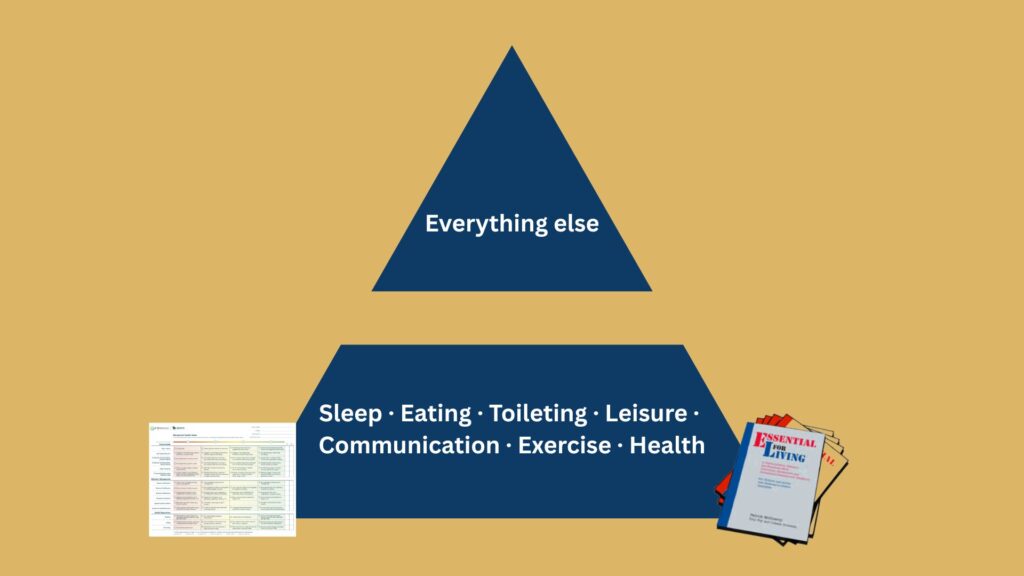
This framework draws directly from the Behavioral Health Index (BHI; developed by Acorn Health and FTF Behavioral Consulting), a structured assessment tool that tracks an individual’s progress across critical skills, behaviour management, and health repertoires. The index rates functioning on a four-point scale, from Level 1 (highly restricted lifestyle, high risk for severe problem behaviour) to Level 4 (unrestricted lifestyle, low risk for severe problem behaviour). Health repertoires — including sleep, eating, and exercise — sit explicitly within the assessment, alongside communication, behaviour management, and social access.
The second framework Renee discussed was Essential for Living (EFL), a framework that has had a significant influence on her day-to-day clinical practice with a particular focus on the Necessary Nine Skills (referred to as the “Essential Eight” in the current EFL manual, with leisure skills now thankfully reinstated as the ninth element). These foundational, high-priority life skills are considered essential for everyone, but particularly for individuals with moderate to severe disabilities and limited skill repertoires. Renee explained that the Necessary Nine include skills such as making requests, waiting, accepting transitions and turn-taking, completing required tasks, accepting “no,” following health and safety directions, completing daily living skills related to health and safety, tolerating health and safety procedures, and engaging in leisure activities. She noted that these skills were specifically identified because their absence is often associated with severe problem behaviour and emphasised their importance in supporting safe, meaningful, and effective participation across family life, school environments, and the broader community.

The message was clear: health behaviours are not supplementary goals. They are among the most clinically important targets we can address.
Sleep. Feeding. Toileting. These Are Behaviours.
One of the most resonant moments of the presentation was a slide that read simply: “Sleep. Feeding. Toileting. These are behaviours. And we are very skilled at behaviour change.”
This reframing matters enormously for practitioners who may see health challenges as outside their scope, or who defer to medical colleagues without first applying a behavioural lens. Renee positioned ABA and behaviour analytic practitioners as uniquely equipped to address these areas — not despite their clinical training, but because of it.
Sleep
Research cited in the presentation shows that 63–80% of autistic children experience behavioural sleep disorders, compared to 35–50% of typically developing peers (Hanley, 2013). The downstream consequences are significant: increased problem behaviour, reduced learning, poor cooperation, and elevated family stress. Sleep is a skill deficit, and all individuals can learn to be better sleepers. This positions sleep intervention not as a medical matter alone, but as a legitimate and important target for behaviour analytic intervention.
Feeding and Diet
The feeding section used an iceberg analogy to powerful effect. What families and referrers present as “picky eating,” food refusal, or mealtime battles is only the visible tip. Beneath the surface lies a complex web of consequences: nutritional deficiency, neurotransmitter disruption, mood dysregulation, anxiety, social exclusion, and behaviour that ripples across the entire day. Renee’s closing line on this slide was particularly pointed: “We are not just expanding a menu.” Food intervention is not about preferences — it is about health, participation, and quality of life.
Toileting
When discussing continence, Renee explored the profound impact that achieving toileting has on a family’s world. Continence opens doors: access to a greater range of education settings, community participation, and independence. The slide was only partially visible in the presentation, but the message was unmistakable — toileting is not a “nice to have.” For many families, it is the skill that changes everything.
What Changes When Families Have Capacity
Renee drew a direct and practical line between health behaviours and a family’s capacity to engage with therapy:
- Better sleep → the child is more available for learning
- Toileting achieved → the family’s world opens up
- A leisure repertoire → problem behaviour becomes less likely to start
These are not abstract benefits. They are the concrete, ripple-on effects of getting health behaviours right early. When practitioners prioritise these foundations, everything else in the intervention becomes more possible.
When Families Don’t Have Capacity
Perhaps the most practically useful part of Renee’s presentation was her guidance on what to do when a family presents with health behaviour needs but doesn’t currently have the capacity to address them. Her three-step approach was compassionate and realistic:
- Name it — raise the issue clearly and compassionately. Don’t avoid it because it feels too hard.
- Hold it — document the concern and set a review date 3–6 months away.
- Find small steps — ask: is there anything we can do right now, even incrementally?
This framework respects the reality that families are often overwhelmed, under-resourced, and not always in a position to take on new programs. But it also refuses to let health behaviour concerns disappear from the clinical picture.
The Closing Challenge
Renee ended her presentation with a call to action that will stay with many in the room. Projected in large text on the final slide, her closing statement was:
“Must-Have skills first. Not because it is dogma — because the families we work with deserve practitioners brave enough to have that conversation at the beginning.”
This is a challenge to every allied health and behaviour support professional to reorder their clinical priorities, to be willing to raise health behaviours with families before diving into skill programs and behaviour plans, and to treat sleep, feeding, toileting, and exercise with the same clinical rigour we bring to everything else.
Renee’s presentation reminded us that the families who access our services are trusting us to see the whole picture, not just the referral reason, but the foundations that either enable or undermine everything we are trying to achieve together.



